The international outbreak of SARS-CoV-2 brought a flurry of activity to the public health programs at University of California, Davis. In addition to mobilizing resources to address the pandemic at a larger scale, the university established a high-throughput monitoring system to protect the local community called Healthy Davis Together (HDT), and later Healthy Yolo Together (HYT). I was recruited as a statistician and a writer for the biostatistics arm of HDT, led by Dr. Miriam Nuño. Her research group took a divide-and-conquer approach, with each project being driven by a different researcher, while everyone consulted on the totality of the work.
Our first research goal was to assess the transmission parameters in California and Yolo County to assure equitable application of mitigation strategies. Early data came from clinical tests at the five UC hospitals and surveillance data from town and the university community. Our first challenge was to repurpose these data to draw conclusions about what health and social factors contributed to underlying transmission dynamics. These are classic problems with emerging diseases: clinical tests are usually used on a population of people who are already ill; and surveillance tests (i.e., mass PCR testing required for work) are more akin to a convenience sample than a random sample.
The Role of SARS-CoV-2 Testing on Hospitalizations in California
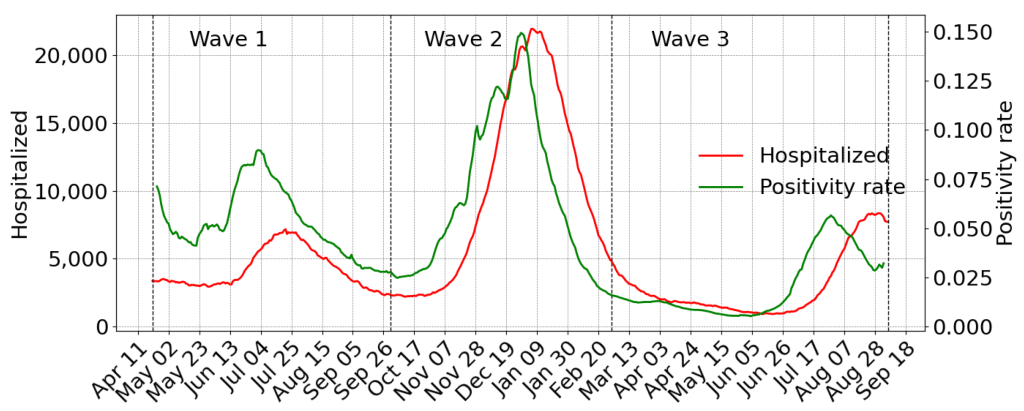
Hospitals were especially overwhelmed by the new year as cases surged into a second wave. With no end to the pandemic in sight, and the mRNA vaccines still a whispered hope, there was a vital need to understand the demand hospitals may see in the future. Though test positivity rate is not a direct measurement of the prevalence of disease, we thought it could still give consistent warning for incoming waves of hospitalizations when properly adjusted for localized populations.
Though the results showed that the clear visual relationship held up quantitatively, it also revealed the the risks to Californians shifted as time went on. This study also represented our first foray into folding the Healthy Places Index (HPI) into our analysis. HPI is an ensemble index measurement of socioeconomic access to healthcare and long-term environmental exposures, produced by the Public Health Alliance of Southern California, made available for free to the public.
My role: writing and editing.
COVID-19 vaccination in California: Are we equitable yet?
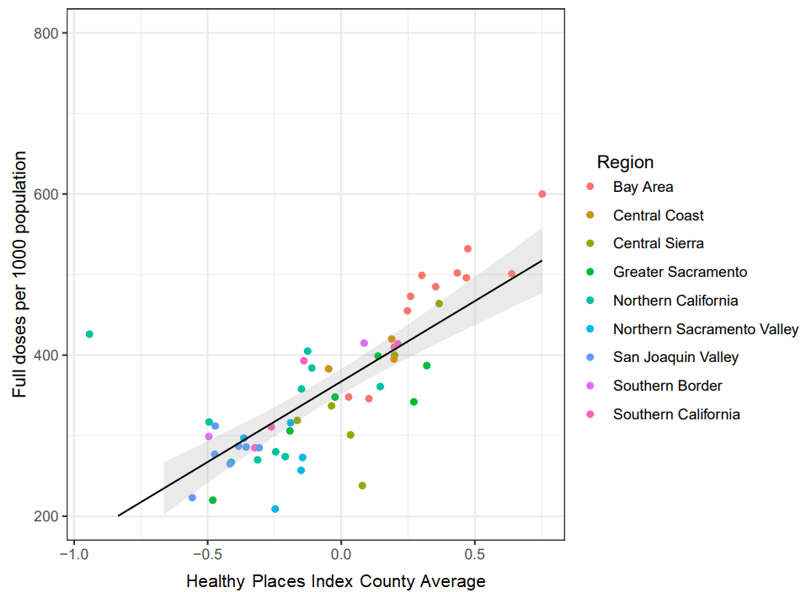
It was March 2021, and the mRNA vaccine had finally been approved and free distribution to the public had begun. Unfortunately, California’s rollout of the vaccine program had a poor start as far as equitable access was concerned, prompting governor Gavin Newsom to apportion millions of doses for people in the counties with the lowest socioeconomic indicators. With the vaccine promising relief in the near future, we were scrambling to ensure that vaccination rates remained equitable and brought everyone the protection they deserved before California lifted the stay-at-home orders on June 15th.
Are we equitable yet? was a research letter that attempted to address this question. While California did show improvements in coverage, we showed that while the average vaccination rates would hit the numbers required for opening up, it was still primarily driven by the 18 counties with the highest HPI and would leave the other 40 counties lagging behind, some quite considerably.
Academic publishing being what it is, unfortunately we could not get this note published before the deadline. We made sure it was available to read online, even if it hadn’t been peer reviewed yet.
My role: conception, design, analysis, writing, and editing.
COVID-19 hospitalizations in five California hospitals: a retrospective cohort study
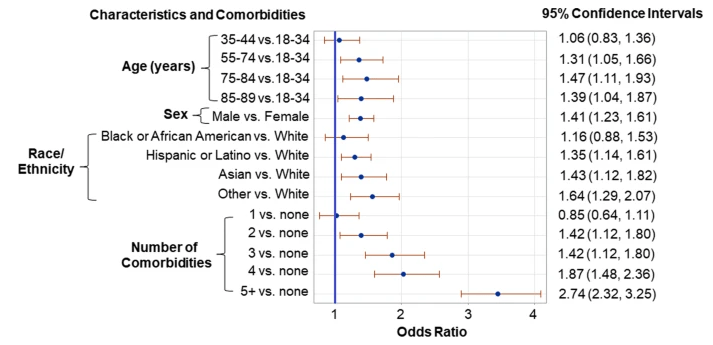
Researchers in the UC system, which featured five teaching hospitals in areas with varied and diverse populations, were positioned well to examine the factors associated with poor outcomes from COVID-19. Based on our previous work with California hospitals and equitable vaccine coverage, Dr. Nuño led the effort to apply rigorous epidemiological investigation that sought to better understand the risk factors for ICU admission and death.
We leveraged data from CORDS (the COVID-19 Research Data Set), assembled by UCSF analysts from the anonymized electronic medical records (EMRs) of patients across the UC health systems. While EMRs lack some details that would allow comparison to a broader population, like socioeconomic information, what they do provide is a detailed accounting of vital statistics and comorbidities at the time of diagnosis.
Looking back on this paper in the (arguably) post-pandemic period reads like a laundry list of things that now feel like common knowledge. At the time, though, it was a relief to confirm much of what was suspected and finally start citing the collected research results to those in policy positions.
My role: writing and editing.
The impact of COVID-19 vaccination on California’s return to normalcy
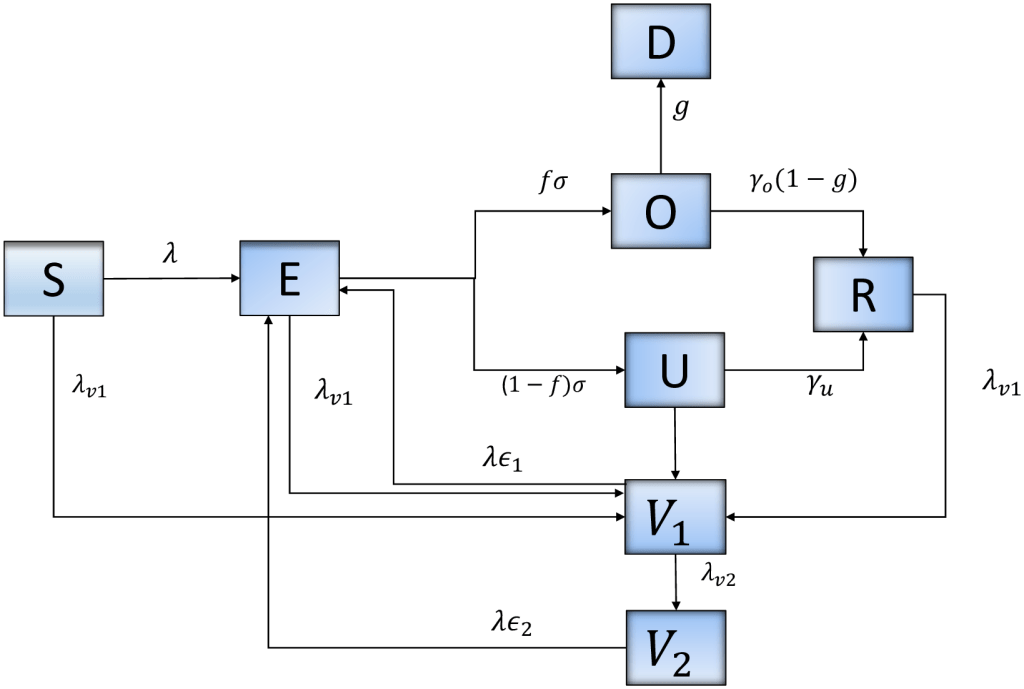
Research narrative here.
Methodology, literature review, writing, and editing.
Model training periods impact estimation of COVID-19 incidence from wastewater viral loads
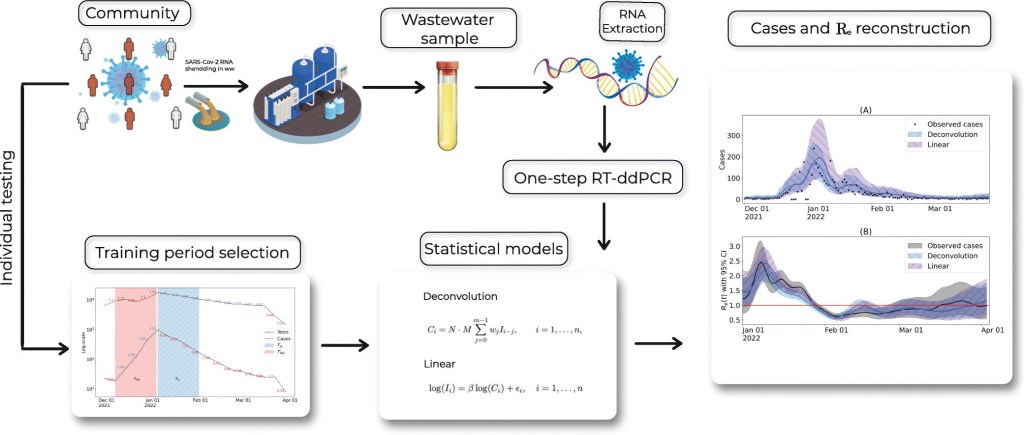
Disease surveillance via large-scale PCR testing is an expensive solution that is unsustainable for long periods of time. Dr. Heather Bischel, an HDT collaborator, recognized that wastewater-based epidemiology (WBE) had great potential for tracking COVID-19 in places where surveillance testing wasn’t feasible. We compared two possible statistical models that related viral nucleotide concentrations from wastewater effluent to incidence in the local community.
Results were promising, displaying accurate measurements when trained in comparison with robust surveillance testing. WBE is much less resource intensive than surveillance testing, but nevertheless requires a strong, targeted sample of clinical tests in the community to avoid underestimating rates of disease transmission.
My role: literature review, writing, and editing.

Leave a comment